LB2. Safety and Efficacy of Combination SARS-CoV-2 Monoclonal Neutralizing Antibodies (mAb) BRII-196 and BRII-198 in Non-Hospitalized COVID-19 Patients
MD Pablo Ryan, PhD Gregory Camus, Gilead, PhD Danielle P Porter, DPhil Robert H Hyland, PhD Shuguang Chen, MD Kavita Juneja, MD Frank Duff, MD Robert L Gottlieb, Eli Lilly, MD Teresa H Evering, Ph.D Mark Giganti, MD Kara W Chew, Ph.D Michael Hughes, Ph.D Carlee Moser, MD David Alain Wohl, M.D Judith Currier, MD Joseph J Eron, M.D Arzhang Javan, M.P.H D T M&h, MD MPH David A Margolis, PhD Qing Zhu, MD Ulises D' Andrea, M.D. 10 Keila Hoover, M.D Bharat R Mocherla, Pharm.D. 12 Courtney Fletcher, M.D Jonathan Li, M.D. 14 Davey Smith, Eric Daar
S807 treatment of patients hospitalized with moderate to severe COVID-19. This Phase 3 (GS-US-540-9012) double-blind, placebo-controlled study compared the efficacy and safety of 3 days of RDV to standard of care in non-hospitalized, high-risk participants with confirmed COVID-19. Table 1. COVID-19 related hospitalization or death, COVID-19 related medically attended visits or death, and Treatment Emergent Adverse Events Methods. Participants were randomly assigned 1:1 to receive intravenous (IV) RDV (200 mg on day 1, 100 mg on days 2 to 3) or placebo. The primary efficacy endpoint was composite COVID-19 hospitalization or all-cause death by day 28 and compared using Cox proportional hazards model with baseline stratification factors as covariates. The primary safety endpoint was proportion of participants with treatment-emergent adverse events. Study enrollment was terminated early for administrative reasons in light of the evolving pandemic. Results. 562 patients underwent randomization and started their assigned treatment (279, RDV; 283, placebo). Baseline demographics and characteristics were balanced across arms. Overall, 52% were male, 44% were Hispanic/Latino ethnicity and 30% were ≥ 60 years old. The most common comorbidities were diabetes mellitus (62%), obesity (56%; median BMI, 30.7), and hypertension (48%). Median baseline SARS-CoV-2 RNA nasopharyngeal viral load was 6.2 log 10 copies/mL. Treatment with RDV significantly reduced COVID-19 hospitalization or all-cause death by day 28 (HR, 0.13; 95% CI, 0.03 -0.59; p = 0.008; Table 1 ) compared to placebo. Participants receiving RDV also had significantly lower risk for COVID-19-related medically attended visits or all-cause death by day 28 compared to placebo (HR, 0.19; 95% CI, 0.07 -0.56; p = 0.002; Table 1 ). No deaths occurred in either arm by day 28. There was no difference between arms in time-weighted average change in nasopharyngeal viral loads from baseline up to day 7. The proportion of patients with AEs was similar between arms (Table 1 ); the most common AEs in the RDV arm were nausea (11%), headache (6%), and diarrhea (4%).
Conclusion. A 3-day course of IV RDV was safe, well tolerated and highly effective at preventing COVID-19 related hospitalization or death in high-risk non-hospitalized COVID-19 patients. Disclosures.
Methods. COV-BARRIER (NCT04421027) was a randomized double-blind, placebo-controlled trial in patients with confirmed SARS-CoV-2 infection and elevation of ≥ 1 serum inflammatory marker. In this newly completed substudy, enrolled participants (not previously reported) from 4 countries on IMV or ECMO at study entry were randomly assigned 1:1 to once-daily BARI 4-mg or placebo (PBO) for up to 14 days plus standard of care (SOC), which included baseline systemic corticosteroid use in 86% of patients. The prespecified exploratory endpoints included all-cause mortality and number of ventilator-free days (VFDs) through Day 28. Results. Characteristics for 101 participants are shown in Table 1 . Treatment with BARI significantly reduced all-cause mortality by Day 28 compared to PBO [39.2% vs 58.0%, respectively; hazard ratio (HR) = 0.54 (95%CI 0.31, 0.96), p=0.030, relative risk (RR) = 0.68 (95%CI 0.45, 1.02); Figure 1A ]. One additional death was prevented for every six BARI-treated patients. Significant reduction in mortality was also observed by Day 60 [45.1% vs 62.0%; HR = 0.56 (95%CI 0.33, 0.97), p=0.027, RR = 0.73 (95%CI 0.50, 1.06); Figure 1B ]. Patients treated with BARI showed a numerical reduction in the duration of IMV and duration of hospitalization vs PBO and more BARI treated patients recovered (Table 2 ). No new safety findings were observed (Table 2 ).
Conclusion. Treatment with BARI+SOC (corticosteroids) resulted in an absolute risk reduction in mortality of..
{ 'indexed': {'date-parts': [[2024, 4, 29]], 'date-time': '2024-04-29T02:18:06Z', 'timestamp': 1714357086503},
'reference-count': 0,
'publisher': 'Oxford University Press (OUP)',
'issue': 'Supplement_1',
'license': [ { 'start': { 'date-parts': [[2021, 12, 4]],
'date-time': '2021-12-04T00:00:00Z',
'timestamp': 1638576000000},
'content-version': 'vor',
'delay-in-days': 33,
'URL': 'https://creativecommons.org/licenses/by/4.0/'}],
'content-domain': {'domain': [], 'crossmark-restriction': False},
'published-print': {'date-parts': [[2021, 12, 4]]},
'abstract': '<jats:title>Abstract</jats:title>\n'
' <jats:sec>\n'
' <jats:title>Background</jats:title>\n'
' <jats:p>SARS-CoV-2 continues to spread and the development of safe and '
'effective therapeutics for the prevention of severe disease remains a priority. BRII-196 and '
'BRII-198 are non-competing anti-SARS-CoV-2 mAbs with YTE triple amino acid substitution in Fc '
'to extend half-life and reduce receptor binding, that are being studied for treatment of '
'COVID-19 in the ACTIV-2 Trial, sponsored by NIAID and led by ACTG.</jats:p>\n'
' </jats:sec>\n'
' <jats:sec>\n'
' <jats:title>Methods</jats:title>\n'
' <jats:p>ACTIV-2 evaluates safety/efficacy of investigational agents for '
'treatment of non-hospitalized adults with mild-moderate COVID-19 under a randomized, blinded, '
'controlled adaptive platform. BRII-196/BRII-198 (1000 mg each) as a single dose given as '
'sequential infusions, or placebo to those at high risk of clinical progression (i.e., age ≥ '
'60 years or presence of other medical conditions) within 10 days of symptom onset and '
'positive test for SARS-CoV-2. The primary endpoint was hospitalization and/or death through '
'day 28. We report Phase 3 BRII-196/BRII-198 trial results per DSMB recommendation following '
'an interim analysis.</jats:p>\n'
' </jats:sec>\n'
' <jats:sec>\n'
' <jats:title>Results</jats:title>\n'
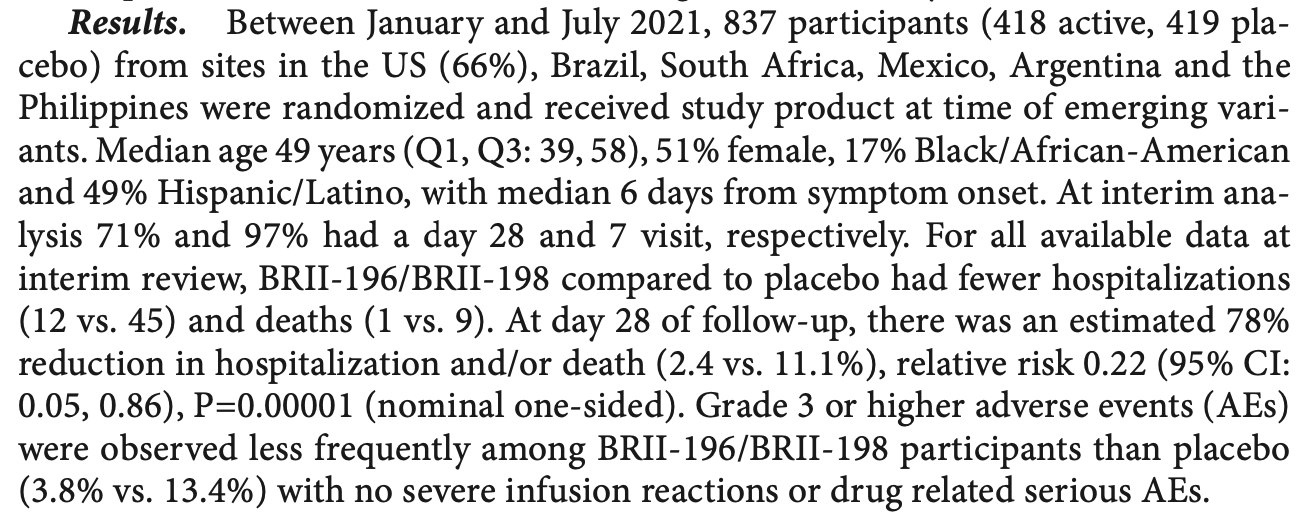
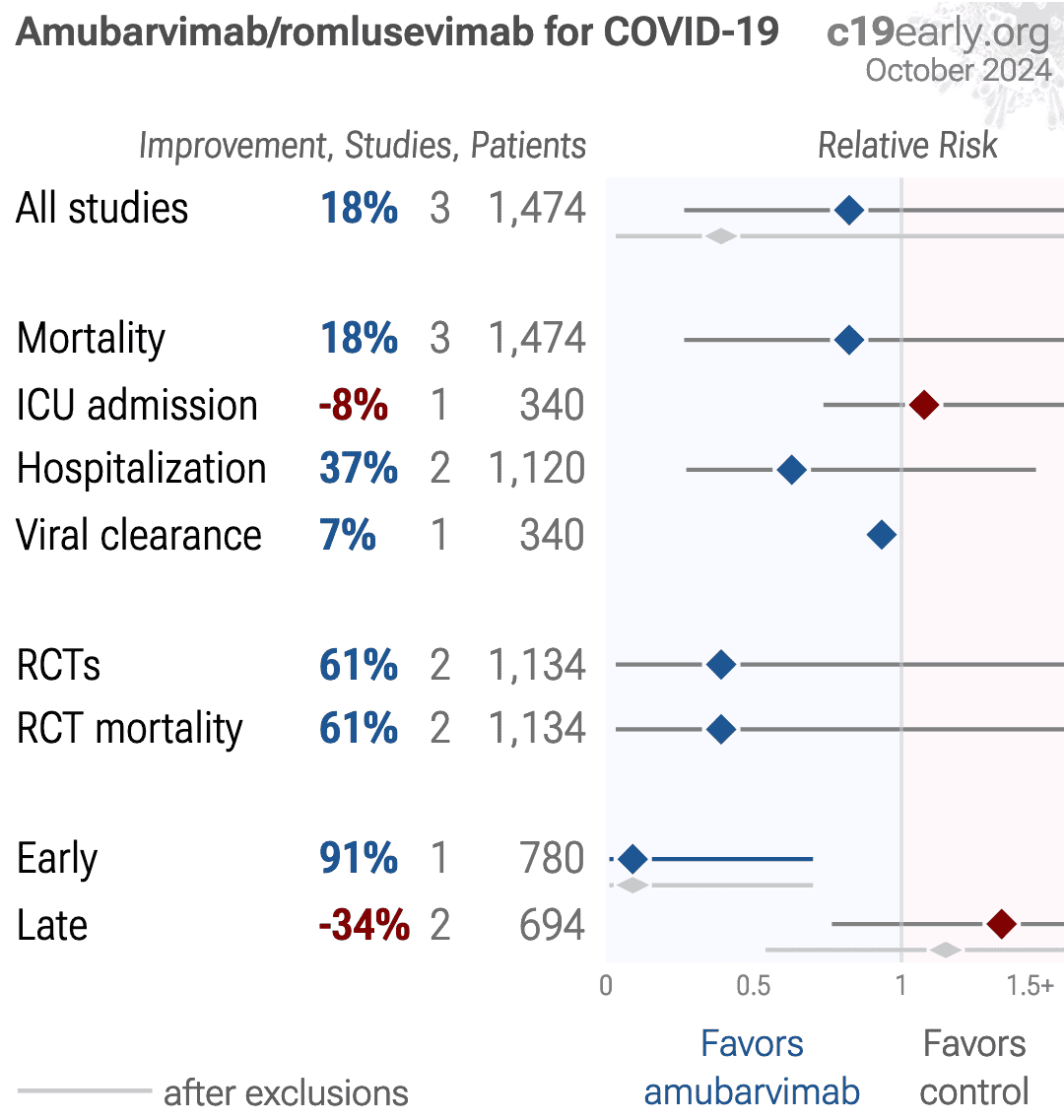
' <jats:p>Between January and July 2021, 837 participants (418 active, 419 '
'placebo) from sites in the US (66%), Brazil, South Africa, Mexico, Argentina and the '
'Philippines were randomized and received study product at time of emerging variants. Median '
'age 49 years (Q1, Q3: 39, 58), 51% female, 17% Black/African-American and 49% '
'Hispanic/Latino, with median 6 days from symptom onset. At interim analysis 71% and 97% had a '
'day 28 and 7 visit, respectively. For all available data at interim review, BRII-196/BRII-198 '
'compared to placebo had fewer hospitalizations (12 vs. 45) and deaths (1 vs. 9). At day 28 of '
'follow-up, there was an estimated 78% reduction in hospitalization and/or death (2.4 vs. '
'11.1%), relative risk 0.22 (95% CI: 0.05, 0.86), P=0.00001 (nominal one-sided). Grade 3 or '
'higher adverse events (AEs) were observed less frequently among BRII-196/BRII-198 '
'participants than placebo (3.8% vs. 13.4%) with no severe infusion reactions or drug related '
'serious AEs.</jats:p>\n'
' </jats:sec>\n'
' <jats:sec>\n'
' <jats:title>Conclusion</jats:title>\n'
' <jats:p>BRII-196/BRII-198 was safe, well-tolerated, and demonstrated '
'significant reduction compared to placebo in the risk of hospitalization and/or death among '
'adults with mild-moderate COVID-19 at high risk for progression to severe disease.</jats:p>\n'
' </jats:sec>\n'
' <jats:sec>\n'
' <jats:title>Disclosures</jats:title>\n'
' <jats:p>Kara W. Chew, MD, MS, Amgen (Individual(s) Involved: Self): '
'Grant/Research Support; Merck Sharp & Dohme (Individual(s) Involved: Self): '
'Grant/Research Support David Alain Wohl, MD, Gilead Sciences (Individual(s) Involved: Self): '
'Advisor or Review Panel member, Consultant, Research Grant or Support, Scientific Research '
'Study Investigator; Janssen (Individual(s) Involved: Self): Advisor or Review Panel member; '
'Merck (Individual(s) Involved: Self): Advisor or Review Panel member, Research Grant or '
'Support; ViiV (Individual(s) Involved: Self): Advisor or Review Panel member, Research Grant '
'or Support Joseph J. Eron, MD, Gilead Sciences (Consultant, Research Grant or Support)Janssen '
'(Consultant, Research Grant or Support)Merck (Consultant)ViiV (Consultant, Research Grant or '
'Support) David A. Margolis, MD MPH, Brii Biosciences (Employee) Courtney Fletcher, Pharm.D., '
'National Institute of Allergy and Infectious Diseases, NIH (Grant/Research Support) Davey '
'Smith, M.D., Linear Therapies, Matrix Biomed, Bayer (Consultant, Shareholder) Eric Daar, '
'Gilead (Consultant, Grant/Research Support)Merck (Consultant)ViiV (Consultant, Grant/Research '
'Support)</jats:p>\n'
' </jats:sec>',
'DOI': '10.1093/ofid/ofab466.1643',
'type': 'journal-article',
'created': {'date-parts': [[2021, 12, 5]], 'date-time': '2021-12-05T10:08:51Z', 'timestamp': 1638698931000},
'page': 'S807-S808',
'source': 'Crossref',
'is-referenced-by-count': 10,
'title': 'LB2. Safety and Efficacy of Combination SARS-CoV-2 Monoclonal Neutralizing Antibodies (mAb) '
'BRII-196 and BRII-198 in Non-Hospitalized COVID-19 Patients',
'prefix': '10.1093',
'volume': '8',
'author': [ { 'given': 'Teresa H',
'family': 'Evering',
'sequence': 'first',
'affiliation': [{'name': 'Weill Cornell Medicine, New York, NY'}]},
{ 'given': 'Mark',
'family': 'Giganti',
'sequence': 'additional',
'affiliation': [ { 'name': 'Harvard T.H. Chan School of Public Health, Boston, '
'Massachusetts'}]},
{ 'given': 'Kara W',
'family': 'Chew',
'sequence': 'additional',
'affiliation': [{'name': 'David Geffen School of Medicine at UCLA'}]},
{ 'given': 'Michael',
'family': 'Hughes',
'sequence': 'additional',
'affiliation': [ { 'name': 'Harvard T.H. Chan School of Public Health, Boston, '
'Massachusetts'}]},
{ 'given': 'Carlee',
'family': 'Moser',
'sequence': 'additional',
'affiliation': [ { 'name': 'Harvard T.H. Chan School of Public Health, Boston, '
'Massachusetts'}]},
{ 'given': 'David Alain',
'family': 'Wohl',
'sequence': 'additional',
'affiliation': [{'name': 'UNC School of Medicine, Chapel Hill, NC'}]},
{ 'given': 'Judith',
'family': 'Currier',
'sequence': 'additional',
'affiliation': [ { 'name': 'David Geffen School of Medicine at University of California, Los '
'Angeles, Los Angeles, California'}]},
{ 'given': 'Joseph J',
'family': 'Eron',
'sequence': 'additional',
'affiliation': [ { 'name': 'University of North Carolina at Chapel Hill, Chapel Hill, North '
'Carolina'}]},
{ 'given': 'Arzhang',
'family': 'Javan',
'sequence': 'additional',
'affiliation': [{'name': 'National Institute of Health, Bethesda, Maryland'}]},
{ 'given': 'David A',
'family': 'Margolis',
'sequence': 'additional',
'affiliation': [{'name': 'Brii Biosciences, Chapel Hill, North Carolina'}]},
{ 'given': 'Qing',
'family': 'Zhu',
'sequence': 'additional',
'affiliation': [{'name': 'Brii Biosciences, Chapel Hill, North Carolina'}]},
{ 'given': 'Ulises',
'family': 'D’Andrea',
'sequence': 'additional',
'affiliation': [{'name': 'Instituto Medico Rio Cuarto, Rio Cuarto, Cordoba, Argentina'}]},
{ 'given': 'Keila',
'family': 'Hoover',
'sequence': 'additional',
'affiliation': [{'name': 'Miami Clinical Research, Miami, Florida'}]},
{ 'given': 'Bharat R',
'family': 'Mocherla',
'sequence': 'additional',
'affiliation': [{'name': 'Las Vegas Medical Research, Las Vegas, Nevada'}]},
{ 'given': 'Courtney',
'family': 'Fletcher',
'sequence': 'additional',
'affiliation': [{'name': 'University of Nebraska, Omaha, Nebraska'}]},
{ 'given': 'Jonathan',
'family': 'Li',
'sequence': 'additional',
'affiliation': [{'name': 'Brigham & Womens Hospital, Boston, Massachusetts'}]},
{ 'given': 'Davey',
'family': 'Smith',
'sequence': 'additional',
'affiliation': [{'name': 'University of California, San Diego, San Diego, California'}]},
{ 'given': 'Eric',
'family': 'Daar',
'sequence': 'additional',
'affiliation': [{'name': 'Weill Cornell Medicine, New York, NY'}]}],
'member': '286',
'published-online': {'date-parts': [[2021, 12, 4]]},
'container-title': 'Open Forum Infectious Diseases',
'original-title': [],
'language': 'en',
'link': [ { 'URL': 'https://academic.oup.com/ofid/article-pdf/8/Supplement_1/S807/41521229/ofab466.1643.pdf',
'content-type': 'application/pdf',
'content-version': 'vor',
'intended-application': 'syndication'},
{ 'URL': 'https://academic.oup.com/ofid/article-pdf/8/Supplement_1/S807/41521229/ofab466.1643.pdf',
'content-type': 'unspecified',
'content-version': 'vor',
'intended-application': 'similarity-checking'}],
'deposited': { 'date-parts': [[2021, 12, 5]],
'date-time': '2021-12-05T10:26:36Z',
'timestamp': 1638699996000},
'score': 1,
'resource': {'primary': {'URL': 'https://academic.oup.com/ofid/article/8/Supplement_1/S807/6450927'}},
'subtitle': [],
'short-title': [],
'issued': {'date-parts': [[2021, 11, 1]]},
'references-count': 0,
'journal-issue': {'issue': 'Supplement_1', 'published-print': {'date-parts': [[2021, 12, 4]]}},
'URL': 'http://dx.doi.org/10.1093/ofid/ofab466.1643',
'relation': {},
'ISSN': ['2328-8957'],
'subject': [],
'published-other': {'date-parts': [[2021, 11, 1]]},
'published': {'date-parts': [[2021, 11, 1]]}}

{kind=link}
{kind=link}